Alignment or overuse problems of the knee structures can lead to strain, irritation, and/or injury of the quadricepsmuscle and tendon. This produces pain, weakness, and swelling of the knee joint.These problems can affect people of all ages but the majority of patients with overuse injuries of the knee (and specifically quadriceps tendonitis) are involved in soccer, volleyball, or running activities.
 Usually , The term tendinopathy is used to cover most tendon injuries. The insertion of a muscle is its lower attachment point. The quadriceps muscles insert at the top of the patella (kneecap). This injury is an overuse injury, as the pain tends to develop gradually over a period of time, rather than at a specific point.
Usually , The term tendinopathy is used to cover most tendon injuries. The insertion of a muscle is its lower attachment point. The quadriceps muscles insert at the top of the patella (kneecap). This injury is an overuse injury, as the pain tends to develop gradually over a period of time, rather than at a specific point.For a first time injury, recovery may take 2 to 3 months. A longer term chronic, recurring injury may need 4 to 6 months. Gradually return to sports specific training. Again depending on severity this may be days, it may be weeks.
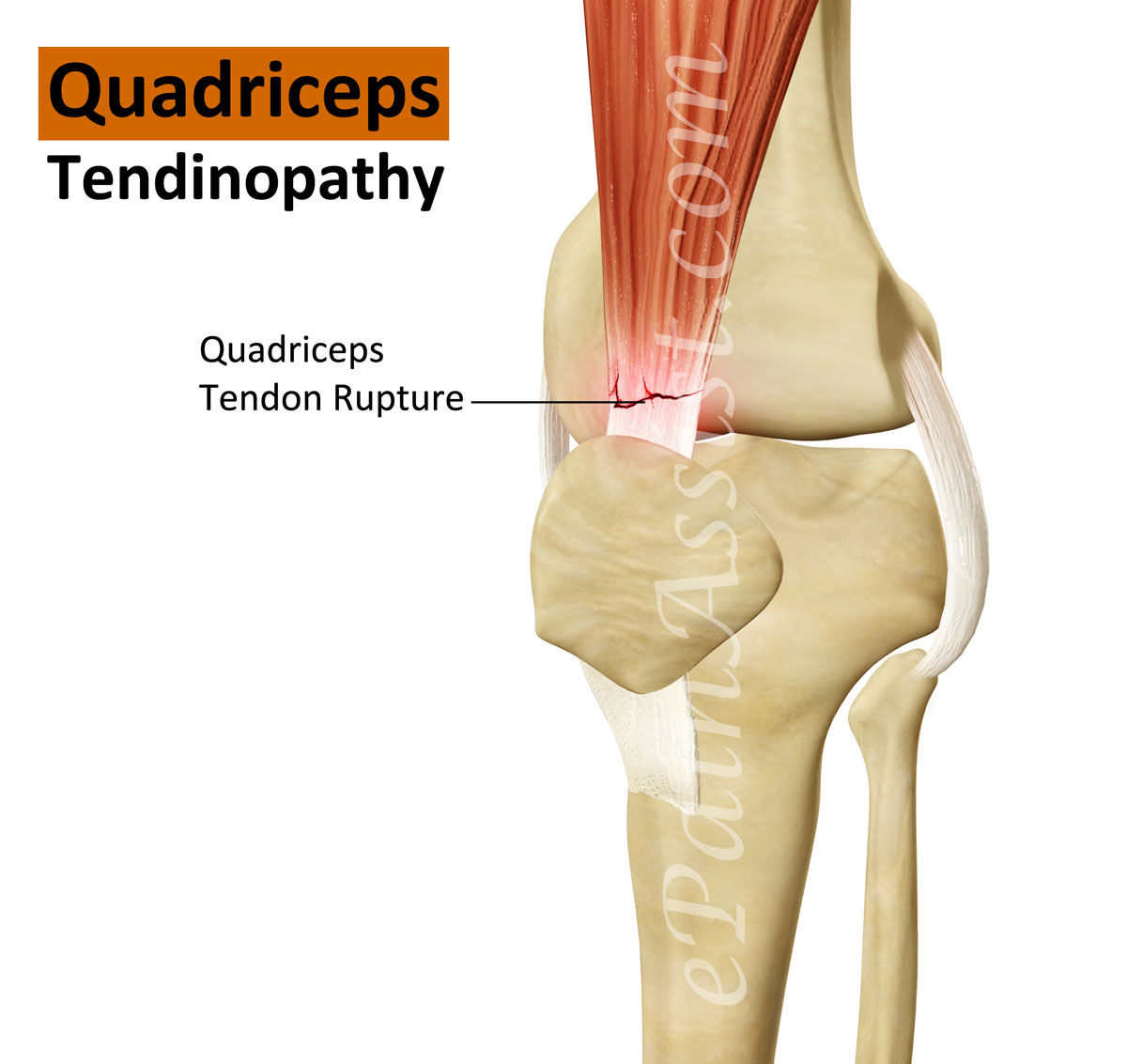
Structure of Quadriceps muscle:
The large quadriceps muscle ends in a tendon that inserts into the tibial tubercle, a bony bump at the top of the tibia (shin bone) just below the patella. The tendon together with the patella is called the quadriceps mechanism. Though we think of it as a single device, the quadriceps mechanism has two separate tendons, the quadriceps tendon on top of the patella and the patellar tendon below the patella. Tightening up the quadriceps muscles places a pull on the tendons of the quadriceps mechanism. This action causes the knee to straighten. The patella acts like a fulcrum to increase the force of the quadriceps muscles.
Causes:
Quadriceps tendonitis occurs most often as a result of stresses placed on the supporting structures of the knee. Running, jumping, and quick starts and stops contribute to this condition. Overuse injuries from sports activities is the most common cause but anyone can be affected, even those who do not participate in sports or recreational activities.
Extrinsic factors: 1) Inappropriate footwear 2) Training error 3) Surface area of the ground
Intrinsic factors: 1) Flexibility, and joint laxity 2) Malalignment of the foot, ankle, and leg.
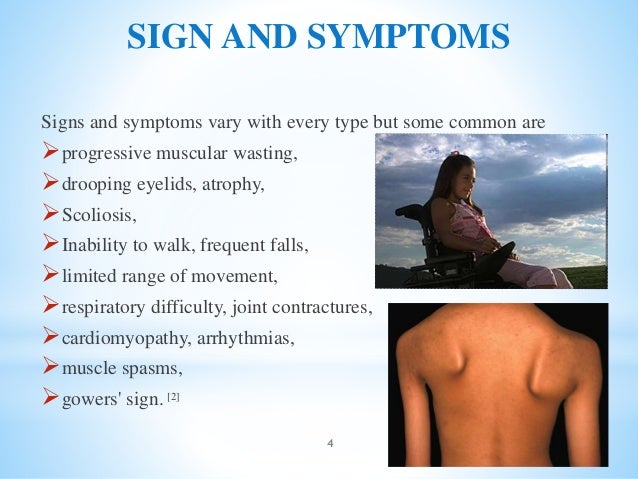
SYMPTOMS:
Pain from quadriceps tendonitis is felt in the area at the bottom of the thigh, just above the patella.

Tenderness develops in the area of the tendon attachment above the kneecap.
May be swelling in and around the quadriceps tendon.
May feel a sense of warmth or burning pain.
Stiffness of the knee is common when you first get up in the morning
PHYSIOTHERAPY MANAGEMENT:
The initial treatment for acute quadriceps tendonitis begins by decreasing the inflammation in the knee.
Physical therapy can help in the early stages by decreasing pain and inflammation. Your physical therapist may use ice massage, electrical stimulation, and ultrasound to limit pain and control (but not completely prevent) swelling. Some amount of inflammatory response is needed for a good healing response. Heat may be used in cases of chronic tendinosis to stimulate blood circulation and promote tissue healing.Your physician may suggest relative rest and anti-inflammatory medications, such as aspirin or ibuprofen.
Relative rest is a term used to describe a process of rest-to-recovery based on the severity of symptoms. Pain at rest means strict rest and a short time of immobilization in a splint or brace is required. When pain is no longer present at rest, then a gradual increase in activity is allowed so long as the resting pain doesn't come back.
The therapist will prescribe stretching and strengthening exercises to correct any muscle imbalances. Flexibility exercises are often designed for the thigh and calf muscles. Specific exercises are used to maximize control and strength of the quadriceps muscles. You will be shown how to ease back into jumping or running sports using good training techniques
Bracing or taping the patella can help you do exercises and activities with less pain. Therapists also design special shoe inserts, called orthotics, to improve knee alignment and function of the patella. Proper footwear for your sport is important. The therapist will advise you in this area.
Prevention of future injuries through patient education is a key component of the treatment program. This is true whether conservative care or surgical intervention is required. Modification of intrinsic and extrinsic risk factors is essential.
Taping:
Kinesiology tape is supposed to last several days, but to achieve this the skin needs to be clean and dry or the tape will peel off. Wash and dry the area thoroughly, and do not apply any oils, lotions or moisturisers
.
Step 2: With the knee bent at 90 degrees, apply the unsplit end of the kinesiology tape down the midpoint of the front thigh. Apply the tape without any stretch. The point where the split begins must be above the kneecap:
Step 3: Fan the split ends of the kinesiology tape around the kneecap. Bring each strip of tape down either side of the kneecap, and then around below it. Again, apply the tape with no stretch. The two split ends should cross each either in the soft area just below the kneecap:
Step 4: Finally, give the kinesiology tape a good rub with the flat of the hands to warm it up and activate the adhesive.
Exercises to improve the condition of Quadriceps Tendinitis:
Static Quads
A static quads contraction is a good beginning exercise for quads tendonitis rehab. There is less risk of experiencing pain or aggravating the knee joint at this stage. Do this exercise by lying or half-sitting on a mat on the floor with legs stretched out in front of you. Place a rolled-up towel underneath your knee. Contract your thigh muscle such that the back of your knee pushes into the towel. Hold for approximately 10 seconds. Release and repeat 10 times for a total of three sets.
Straight Leg Raise
The straight leg raise exercise strengthens the quadriceps muscle on the front of the thigh. Do this exercise by lying on your back on a mat. Lift your leg up into the air approximately 5 to 10 inches and hold for ten seconds. Return to start and repeat 10 to 12 times for a total of three sets.
Quads Stretch

Stretching the quadriceps muscle will help release tight structures and increase flexibility. Bend your affected leg up and grab your ankle with the hand on the same side of the body. Lift your ankle up toward your buttocks until you feel a stretch on the front of the thigh. Hold for approximately 20 to 30 seconds and repeat two to three times. Avoid bending forward at the waist during this exercise, which will take the emphasis of the stretch off the quad muscles.
Considerations for exercises:
Exercises for quadriceps tendonitis should be performed pain-free. If you are experiencing pain or an increase in pain, you may need to back off exercises or rest more. Consult with a physiotherapist who can advise you on how to treat your injury. Furthermore, your exercise program should consist of core-, gluteal- and hip-strengthening exercises to strengthen surrounding and supporting muscles and prevent muscular imbalances. Thank you.